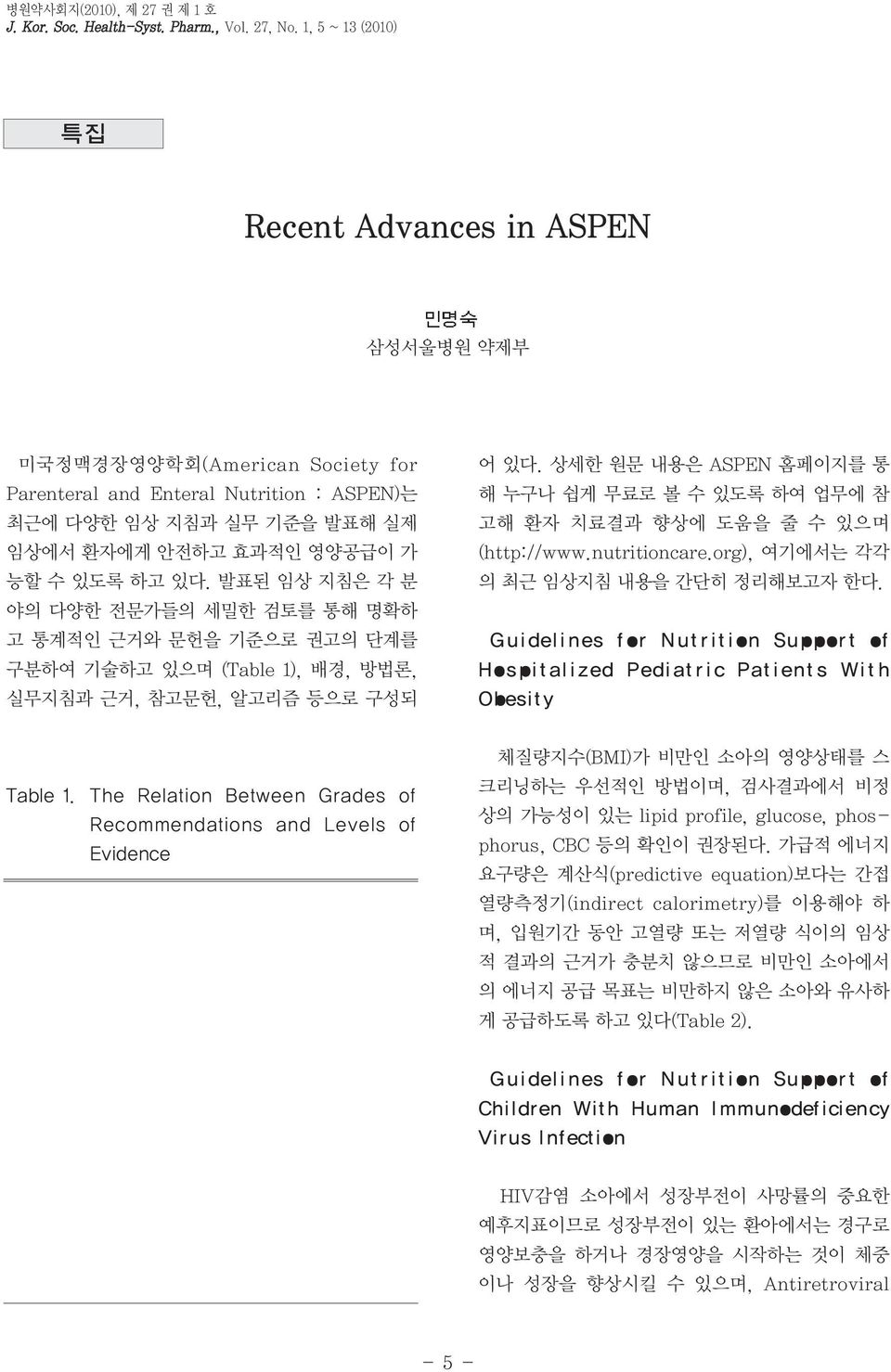
병원약사회지(2010), 제 27 권 제 1 호 J. Kor. Soc. Health-Syst. Pharm., Vol. 27, No. 1, 5 ~ 13 (2010) 특집 Recent Advances in ASPEN 삼성서울병원 약제부 미국정맥경장영양학회(American Society for Parenteral and Enteral Nutrition : ASPEN)는 최근에 다양한 임상 지침과 실무 기준을 발표해 실제 임상에서 환자에게 안전하고 효과적인 영양공급이 가 능할 수 있도록 하고 있다. 발표된 임상 지침은 각 분 야의 다양한 전문가들의 세밀한 검토를 통해 명확하 고 통계적인 근거와 문헌을 기준으로 권고의 단계를 구분하여 기술하고 있으며 (Table 1), 배경, 방법론, 실무지침과 근거, 참고문헌, 알고리즘 등으로 구성되 어 있다. 상세한 원문 내용은 ASPEN 홈페이지를 통 해 누구나 쉽게 무료로 볼 수 있도록 하여 업무에 참 고해 환자 치료결과 향상에 도움을 줄 수 있으며 (http://www.nutritioncare.org), 여기에서는 각각 의 최근 임상지침 내용을 간단히 정리해보고자 한다. Guidelines for Nutrition Support of Hospitalized Pediatric Patients With Obesity Table 1. The Relation Between Grades of Recommendations and Levels of Evidence 체질량지수(BMI)가 비만인 소아의 영양상태를 스 크리닝하는 우선적인 방법이며, 검사결과에서 비정 상의 가능성이 있는 lipid profile, glucose, phosphorus, CBC 등의 확인이 권장된다. 가급적 에너지 요구량은 계산식(predictive equation)보다는 간접 열량측정기(indirect calorimetry)를 이용해야 하 며, 입원기간 동안 고열량 또는 저열량 식이의 임상 적 결과의 근거가 충분치 않으므로 비만인 소아에서 의 에너지 공급 목표는 비만하지 않은 소아와 유사하 게 공급하도록 하고 있다(Table 2). Guidelines for Nutrition Support of Children With Human Immunodeficiency Virus Infection HIV감염 소아에서 성장부전이 사망률의 중요한 예후지표이므로 성장부전이 있는 환아에서는 경구로 영양보충을 하거나 경장영양을 시작하는 것이 체중 이나 성장을 향상시킬 수 있으며, Antiretroviral - 5 -
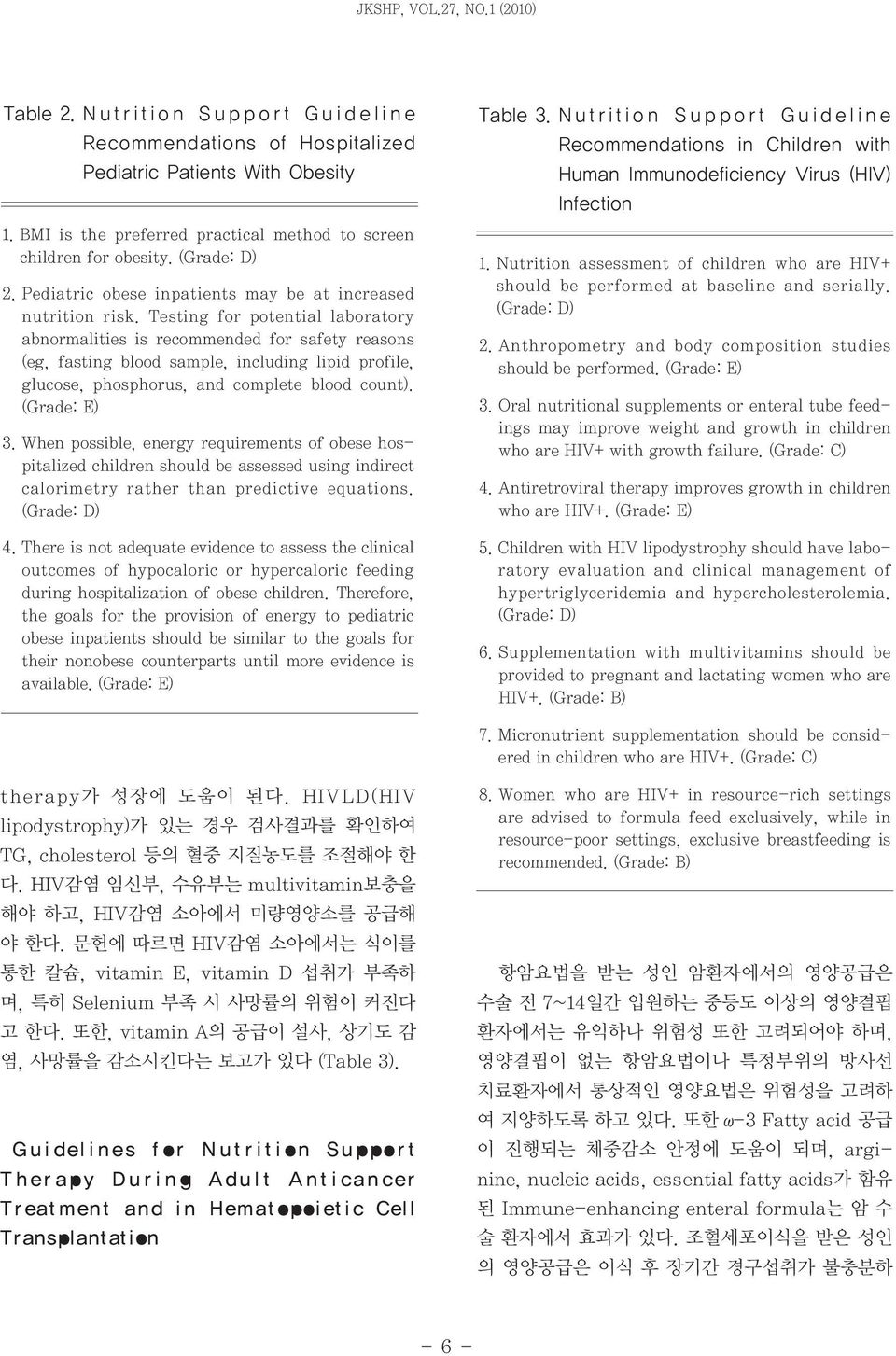
JKSHP, VOL.27, NO.1 (2010) Table 2. Nutrition Support Guideline Recommendations of Hospitalized Pediatric Patients With Obesity 1. BMI is the preferred practical method to screen children for obesity. (Grade: D) 2. Pediatric obese inpatients may be at increased nutrition risk. Testing for potential laboratory abnormalities is recommended for safety reasons (eg, fasting blood sample, including lipid profile, glucose, phosphorus, and complete blood count). 3. When possible, energy requirements of obese hospitalized children should be assessed using indirect calorimetry rather than predictive equations. (Grade: D) 4. There is not adequate evidence to assess the clinical outcomes of hypocaloric or hypercaloric feeding during hospitalization of obese children. Therefore, the goals for the provision of energy to pediatric obese inpatients should be similar to the goals for their nonobese counterparts until more evidence is available. Table 3. N u trition Support Guideline Recommendations in Children with Human Immunodeficiency Virus (HIV) Infection 1. Nutrition assessment of children who are HIV+ should be performed at baseline and serially. (Grade: D) 2. Anthropometry and body composition studies should be performed. 3. Oral nutritional supplements or enteral tube feedings may improve weight and growth in children who are HIV+ with growth failure. 4. Antiretroviral therapy improves growth in children who are HIV+. 5. Children with HIV lipodystrophy should have laboratory evaluation and clinical management of hypertriglyceridemia and hypercholesterolemia. (Grade: D) 6. Supplementation with multivitamins should be provided to pregnant and lactating women who are HIV+. (Grade: B) 7. Micronutrient supplementation should be considered in children who are HIV+. therapy가 성장에 도움이 된다. HIVLD(HIV lipodystrophy)가 있는 경우 검사결과를 확인하여 TG, cholesterol 등의 혈중 지질농도를 조절해야 한 다. HIV감염 임신부, 수유부는 multivitamin보충을 해야 하고, HIV감염 소아에서 미량영양소를 공급해 야 한다. 문헌에 따르면 HIV감염 소아에서는 식이를 통한 칼슘, vitamin E, vitamin D 섭취가 부족하 며, 특히 Selenium 부족 시 사망률의 위험이 커진다 고 한다. 또한, vitamin A의 공급이 설사, 상기도 감 염, 사망률을 감소시킨다는 보고가 있다 (Table 3). Guidelines for Nutrition Support Therapy During Adult Anticancer Treat ment and in Hemat opoiet ic Cell Transplantation 8. Women who are HIV+ in resource-rich settings are advised to formula feed exclusively, while in resource-poor settings, exclusive breastfeeding is recommended. (Grade: B) 항암요법을 받는 성인 암환자에서의 영양공급은 수술 전 7~14일간 입원하는 중등도 이상의 영양결핍 환자에서는 유익하나 위험성 또한 고려되어야 하며, 영양결핍이 없는 항암요법이나 특정부위의 방사선 치료환자에서 통상적인 영양요법은 위험성을 고려하 여 지양하도록 하고 있다. 또한 ω-3 Fatty acid 공급 이 진행되는 체중감소 안정에 도움이 되며, arginine, nucleic acids, essential fatty acids가 함유 된 Immune-enhancing enteral formula는 암 수 술 환자에서 효과가 있다. 조혈세포이식을 받은 성인 의 영양공급은 이식 후 장기간 경구섭취가 불충분하 - 6 -
민명숙 : Recent Advances in ASPEN Table 4. N u trition Support Guideline Recommendations During Adult Anticancer Treatment and in Hematopoietic Cell Transplantation A. Nutrition Support Therapy During Anticancer Treatment 1. Patients with cancer are nutritionally-at-risk and should undergo nutrition screening to identify those who require formal nutrition assessment with development of a nutrition care plan. (Grade: D) 2. Nutrition support therapy should not be used routinely in patients undergoing major cancer operations. (Grade: A) 3. Perioperative nutrition support therapy may be beneficial in moderately or severely malnourished patients if administered for 7-14 days preoperatively, but the potential benefits of nutrition support must be weighed against the potential risks of the nutrition support therapy itself and of delaying the operation. (Grade: A) 4. Nutrition support therapy should not be used routinely as an adjunct to chemotherapy. (Grade: B) 5. Nutrition support therapy should not be used routinely in patients undergoing head and neck, abdominal, or pelvic irradiation. (Grade: B) 6. Nutrition support therapy is appropriate in patients receiving active anticancer treatment who are malnourished and who are anticipated to be unable to ingest and/or absorb adequate nutrients for a prolonged period of time. (Grade: B) 7. The palliative use of nutrition support therapy in terminally ill cancer patients is rarely indicated. (Grade: B) 8. ω-3 Fatty acid supplementation may help stabilize weight in cancer patients on oral diets experiencing progressive, unintentional weight loss. (Grade: B) 9. Patients should not use therapeutic diets to treat cancer. 10. Immune enhancing enteral formulas containing mixtures of arginine, nucleic acids, and essential fatty acids may be beneficial in malnourished patients undergoing major cancer operations. (Grade: A) B. Nutrition Support Therapy in Hematopoietic Cell Transplantation 1. All patients undergoing hematopoietic cell transplantation with myeloablative conditioning regimens are at nutrition risk and should undergo nutrition screening to identify those who require formal nutrition assessment with development of a nutrition care plan. (Grade: D) 2. Nutrition support therapy is appropriate in patients undergoing hematopoietic cell transplantation who are malnourished and who are anticipated to be unable to ingest and/or absorb adequate nutrients for a prolonged period of time (see Guideline 6 Rationale for discussion of "prolonged period of time"). When parenteral nutrition is used, it should be discontinued as soon as toxicities have resolved after stem cell engraftment. (Grade: B) 3. Enteral nutrition should be used in patients with a functioning gastrointestinal tract in whom oral intake is inadequate to meet nutrition requirements. 4. Pharmacologic doses of parenteral glutamine may benefit patients undergoing hematopoietic cell transplantation.* 5. Patients should receive dietary counseling regarding foods which may pose infectious risks and safe food handling during the period of neutropenia. 6. Nutrition support therapy is appropriate for patients undergoing hematopoietic cell transplantation who develop moderate to severe graft-vshost disease accompanied by poor oral intake and/or significant malabsorption. 거나 현격한 흡수장애가 있는 중등도 이상의 GVHD 환자에게 적절하며, 위장관 기능은 있으나 경구섭취 가 충분치 않은 경우에는 경장영양이 우선적으로 고 려되어야 한다. 또한 glutamine의 정맥투여는 질소 평형, 재원기간 및 이환율 감소, 심각한 점막염 감소 에 이점이 있다(Table 4). - 7 -
JKSHP, VOL.27, NO.1 (2010) Table 5. Nutrition Support Guideline Recommendations of the Critically Ill Child 1.1A) Children admitted with critical illnesses should undergo nutrition screening to identify those with existing malnutrition or those who are nutritionally at-risk. (Grade D) 1B) Formal nutrition assessment with the development of a nutrition care plan should be required, especially in those children with premorbid malnutrition. (Grade E) 2.2A) Energy expenditure should be assessed throughout the course of illness to determine the energy needs of critically ill children. Estimates of energy expenditure using available standard equations are often unreliable. (Grade D) 2B) In a subgroup of patients with suspected metabolic alterations or malnutrition, accurate measurement of energy expenditure using indirect calorimetry (IC) is desirable. If IC is not feasible or available, initial energy provision may be based on published formulas or nomograms. Attention to imbalance between energy intake and expenditure will help to prevent overfeeding and underfeeding in this population. (Grade E) 3. There are insufficient data to make evidence-based recommendations for macronutrient intake in critically ill children. After determination of energy needs for the critically ill child, the rational partitioning of the major substrates should be based upon basic understanding of protein metabolism and carbohydrate- and lipid-handling during critical illness. (Grade E) 4. 4A) In critically ill children with a functioning gastrointestinal tract, enteral nutrition (EN) should be the preferred mode of nutrient provision, if tolerated. (Grade C) 4B) A variety of barriers to EN exist in the PICU. Clinicians must identify and prevent avoidable interruptions to EN in critically ill children. (Grade D) 4C) There are insufficient data to recommend the appropriate site (gastric vs post-pyloric/transpyloric) for enteral feeding in critically ill children. Post-pyloric or transpyloric feeds may improve caloric intake when compared to gastric feeds. Nutrition Support of the Critically Ill Child Post-pyloric feeding may be considered in children at high risk of aspiration or those who have failed a trial of gastric feeding. (Grade C) 5. Based on the available pediatric data, the routine use of immunonutrition or immune-enhancing diets/nutrients in critically ill children is not recommended. (Grade D) 6. A specialized nutrition support team in the PICU and aggressive feeding protocols may enhance the overall delivery of nutrition, with shorter time to goal nutrition, increased delivery of EN, and decreased use of parenteral nutrition. The effect of these strategies on patient outcomes has not been demonstrated. (Grade E) 소아 중환자에서 에너지 요구량의 추정식은 종종 신뢰할 수 없음을 염두에 두어야 하며, 대사적 변화 나 영양결핍이 의심되는 경우 간접 열량측정기 (indirect calorimetry) 사용이 바람직하다. 간접 열 량측정기 사용이 어려운 경우 초기 영양공급은 인증 된 계산식이나 nomogram을 사용토록 하며, 과영양 및 저영양 공급 등 영양 불균형이 되지 않도록 주의 해야 한다. 또한, 위장관의 기능이 문제없는 경우 경 장영양을 우선적으로 고려해야 하며, 특히 소아중환 자실 의사는 경장영양 공급에 차질이 생기지 않도록 해야 한다. 경장영양의 적절한 공급경로에 대해 충분 한 자료는 없으나 Post-pyloric, transpyloric feeding이 gastric feeding보다 칼로리 공급을 충분 히할수있어권장되며 Post-pyloric feeding은 흡 인위험이 높거나 gastric feeding이 실패한 환아에 서 고려될 수 있다. 면역 강화 식이의 보편적인 사용 은 추천하고 있지 않으며, 소아 중환자실에서의 영양 지원팀 구성 및 적극적인 영양 프로토콜이 영양공급 을 향상시키고 영양목표에 도달하는 시간을 단축시 키며 TPN 사용을 줄이는 등 전반적으로 도움이 된다 (Table 5). - 8 -
민명숙 : Recent Advances in ASPEN Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient. 중환자에 있어서 영양은 보조적인 역할에서(nutritional support)에서 치료적인 역할로써(nutritional therapy) 조기의 적극적인 영양공급을 권장 하고 있다. 중환자실 입실 이전에 영양결핍의 증거가 없는 건강했던 환자에서는 7일 내 경장영양이 어려운 경우 7일 후에 정맥영양을 하도록 하며, 영양결핍이 있으며 경장영양이 어려운 환자는 정맥영양을 가능 한 빨리 시작하는 것이 적절하다고 제시하고 있다. 열량 요구량은 가급적 간접 열량측정기(indirect calorimetry)를 사용하고, 비만인 중환자에서의 경 장영양 및 중환자에서의 정맥영양은 초기에 열량공 급이 과다해지지 않도록 한다. 정맥영양 공급초기에 는 에너지 요구량의 80% 정도로 공급하는 것이 적절 하고 glutamine 0.5g/kg/day 투여가 사망률, 감염 관련 합병증 발생률을 낮추고 재원기간을 감소시키 는 효과가 있음을 강조하여 강력히 추천하고 있으며, 혈당은 110~150mg/dl를 유지하여 패혈증, 재원기 간, 사망률을 낮추도록 하고, 항산화 비타민 및 selenium을 비롯한 미량원소의 공급이 필요함을 언 급하고 있다. 경장영양은 중환자실 입실 후 24~48 시간 내에 빨리 시작해야 하며, 위 잔여량이 500ml 이하이고 불내성(intolerance)의 다른 증후가 없다 면 자동 중지할 필요는 없고 연구 결과 위 잔여량 250~500ml에서도 역류, 흡인, 폐렴 등의 합병증 위 험이 증가하지 않았다는 보고가 있다. ICU 입원환자 라고 해서 Immune-modulating formula를 사용 할 필요는 없으나 ARDS 또는 중증의 급성 폐 손상, 패혈증 환자에서는 ω-3 fish oil, borage oil, 항산 화제가 포함된 formula를 사용하는 것이 재원이나 인공호흡기 사용기간을 줄이고, organ failure, 사 망률을 감소시킨다고 보고하고 있다(Table 6). Table 6. Nutrition Support Guideline Recommendations A. Initiate Enteral Feeding A1. Traditional nutrition assessment tools (albumin, prealbumin, and anthropometry) are not validated in critical care. Before initiation of feedings, assessment should include evaluation of weight loss and previous nutrient intake prior to admission, level of disease severity, comorbid conditions, and function of the gastrointestinal tract. A2. Nutrition support therapy in the form of enteral nutrition (EN) should be initiated in the critically ill patient who is unable to maintain volitional intake. A3. EN is the preferred route of feeding over parenteral nutrition (PN) for the critically ill patient who requires nutrition support therapy. (Grade: B) A4. Enteral feeding should be started early within the first 24-48 hours following admission. The feedings should be advanced toward goal over the next 48-72 hours. A5. In the setting of hemodynamic compromise (patients requiring significant?hemodynamic support including high dose catecholamine agents, alone or in combination with large volume fluid or blood product resuscitation to maintain cellular perfusion), EN should be withheld until the patient is fully resuscitated and/or stable. A6. In the ICU patient population, neither the presence nor absence of bowel sounds nor evidence of passage of flatus and stool is required for the initiation of enteral feeding. (Grade: B) A7. Either gastric or small bowel feeding is acceptable in the ICU setting. Critically ill patients should be fed via an enteral access tube placed in the small bowel if at high risk for aspiration or after showing intolerance to gastric feeding. Withholding of enteral feeding for repeated high gastric residual volumes alone may be sufficient reason to switch to small bowel feeding (the definition for high gastric residual volume is likely to vary from one hospital to the next, as determined by individual institutional protocol). (See guideline D4 for recommendations on gastric - 9 -
JKSHP, VOL.27, NO.1 (2010) residual volumes, identifying high risk patients, and reducing chances for aspiration.) B. When to Use Parenteral Nutrition B1. If early EN is not feasible or available the first 7 days following admission to the ICU, no nutrition support therapy (ie, STD therapy) should be provided. In the patient who was previously healthy prior to critical illness with no evidence of protein-calorie malnutrition, use of PN should be reserved and initiated only after the first 7 days of hospitalization (when EN is not available). B2. If there is evidence of protein-calorie malnutrition on admission and EN is not feasible, it is appropriate to initiate PN as soon as possible following admission and adequate resuscitation. B3. If a patient is expected to undergo major upper GI surgery and EN is not feasible, PN should be provided under very specific conditions: If the patient is malnourished, PN should be initiated 5-7 days preoperatively and continued into the postoperative period. (Grade: B) PN should not be initiated in the immediate postoperative period but should be delayed for 5-7 days (should EN continue not to be feasible). (Grade: B) PN therapy provided for a duration of <5-7 days would be expected to have no outcome effect and may result in increased risk to the patient. Thus, PN should be initiated only if the duration of therapy is anticipated to be 7 days. (Grade: B) C. Dosing of Enteral Feeding C1. The target goal of EN (defined by energy requirements) should be determined and clearly identified at the time of initiation of nutrition support therapy. Energy requirements may be calculated by predictive equations or measured by indirect calorimetry. Predictive equations should be used with caution, as they provide a less accurate measure of energy requirements than indirect calorimetry in the individual patient. In the obese patient, the predictive equations are even more problematic without availability of indirect calorimetry. C2. Efforts to provide >50%-65% of goal calories should be made in order to achieve the clinical benefit of EN over the first week of hospitalization. C3. If unable to meet energy requirements (100% of target goal calories) after 7-10 days by the enteral route alone, consider initiating supplemental PN. Initiating supplemental PN prior to this 7-10 day period in the patient already receiving EN does not improve outcome and may be detrimental to the patient. C4. Ongoing assessment of adequacy of protein provision should be performed. The use of additional modular protein supplements is a common practice, as standard enteral formulations tend to have a high non-protein calorie:nitrogen ratio. In patients with body mass index (BMI) <30, protein requirements should be in the range of 1.2-2.0 g/kg actual body weight per day, and may likely be even higher in burn or multi-trauma patients. C5. In the critically ill obese patient, permissive underfeeding or hypocaloric feeding with EN is recommended. For all classes of obesity where BMI is >30, the goal of the EN regimen should not exceed 60%-70% of target energy requirements or 11-14 kcal/kg actual body weight per day (or 22-25 kcal/kg ideal body weight per day). Protein should be provided in a range 2.0 g/kg ideal body weight per day for Class I and II patients (BMI 30-40), 2.5 g/kg ideal body weight per day for Class III (BMI >40). Determining energy requirements is discussed in guideline C1.(Grade: D) D. Monitoring Tolerance and Adequacy of Enteral Nutrition D1. In the ICU setting, evidence of bowel motility (resolution of clinical ileus) is not required in order to initiate EN in the ICU. D2. Patients should be monitored for tolerance of EN (determined by patient complaints of pain and/or distention, physical exam, passage of flatus and stool, abdominal radiographs). Inappropriate cessation of EN should be avoided. Holding EN for gastric residual volumes <500 ml in the absence of other signs of intolerance should be avoided. (Grade: B) The time period that a patient is made nil per os (NPO) prior to, during, and immediately following the - 10-
민명숙 : Recent Advances in ASPEN time of diagnostic tests or procedures should be minimized to prevent inadequate delivery of nutrients and prolonged periods of ileus. Ileus may be propagated by NPO status. D3. Use of enteral feeding protocols increases the overall percentage of goal calories provided and should be implemented. D4. Patients placed on EN should be assessed for risk of aspiration. Steps to reduce risk of aspiration should be employed. The following measures have been shown to reduce risk of aspiration: In all intubated ICU patients receiving EN, the head of the bed should be elevated 30-45. For high-risk patients or those shown to be intolerant to gastric feeding, delivery of EN should be switched to continuous infusion. (Grade: D) Agents to promote motility such as prokinetic drugs (metoclopramide and erythromycin) or narcotic antagonists (naloxone and alvimopan) should be initiated where clinically feasible. Diverting the level of feeding by post-pyloric tube placement should be considered. Use of chlorhexidine mouthwash twice a day should be considered to reduce risk of ventilator-associated pneumonia. D5. Blue food coloring and glucose oxidase strips, as surrogate markers for aspiration, should not be used in the critical care setting. D6. Development of diarrhea associated with enteral tube feedings warrants further evaluation for etiology. E. Selection of Appropriate Enteral Formulation E1. Immune-modulating enteral formulations (supplemented with agents such as arginine, glutamine, nucleic acid, ω-3 fatty acids, and antioxidants) should be used for the appropriate patient population (major elective surgery, trauma, burns, head and neck cancer, and critically ill patients on mechanical ventilation), with caution in patients with severe sepsis. (For surgical ICU patients, Grade: A) (For medical ICU patients, Grade: B) ICU patients not meeting criteria for immunemodulating formulations should receive standard enteral formulations. (Grade: B) E2. Patients with ARDS and severe acute lung injury (ALI) should be placed on an enteral formulation characterized by an anti-inflammatory lipid profile (ie, ω-3 fish oils, borage oil) and antioxidants. (Grade: A) E3. To receive optimal therapeutic benefit from the immune-modulating formulations, at least 50%- 65% of goal energy requirements should be delivered.(grade: C) E4. If there is evidence of diarrhea, soluble fibercontaining or small peptide formulations may be utilized. F. Adjunctive Therapy F1. Administration of probiotic agents has been shown to improve outcome (most consistently by decreasing infection) in specific critically ill patient populations involving transplantation, major abdominal surgery, and severe trauma. No recommendation can currently be made for use of probiotics in the general ICU population due to a lack of consistent outcome effect. It appears that each species may have different effects and variable impact on patient outcome, making it difficult to make broad categorical recommendations. Similarly, no recommendation can currently be made for use of probiotics in patients with severe acute necrotizing pancreatitis, based on the disparity of evidence in the literature and the heterogeneity of the bacterial strains utilized. F2. A combination of antioxidant vitamins and trace minerals (specifically including selenium) should be provided to all critically ill patients receiving specialized nutrition therapy. (Grade: B) F3. The addition of enteral glutamine to an EN regimen (not already containing supplemental glutamine) should be considered in burn, trauma, and mixed ICU patients. (Grade: B) F4. Soluble fiber may be beneficial for the fully resuscitated, hemodynamically stable critically ill patient receiving EN who develops diarrhea. Insoluble fiber should be avoided in all critically ill patients. Both soluble and insoluble fiber should - 11 -
JKSHP, VOL.27, NO.1 (2010) be avoided in patients at high risk for bowel ischemia or severe dys-motility. G. When Indicated, Maximize Efficacy of Parenteral Nutrition G1. If EN is not available or feasible, the need for PN therapy should be evaluated (see guidelines B1, B2, B3, C3). If the patient is deemed to be a candidate for PN, steps to maximize efficacy (regarding dose, content, monitoring, and choice of supplemental additives) should be used. (Grade: C) G2. In all ICU patients receiving PN, mild permissive underfeeding should be considered at least initially. Once energy requirements are determined, 80% of these requirements should serve as the ultimate goal or dose of parenteral feeding. Eventually, as the patient stabilizes, PN may be increased to meet energy requirements. For obese patients (BMI 30), the dose of PN with regard to protein and caloric provision should follow the same recommendations given for EN in guideline C5. (Grade: D) G3. In the first week of hospitalization in the ICU, when PN is required and EN is not feasible, patients should be given a parenteral formulation without soy-based lipids. (Grade: D) G4. A protocol should be in place to promote moderately strict control of serum glucose when providing nutrition support therapy. (Grade: B) A range of 110-150 mg/dl may be most appropriate. G5. When PN is used in the critical care setting, consideration should be given to supplementation with parenteral glutamine. G6. In patients stabilized on PN, periodically repeated efforts should be made to initiate EN. As tolerance improves and the volume of EN calories delivered increases, the amount of PN calories supplied should be reduced. PN should not be terminated until 60% of target energy requirements are being delivered by the enteral route. H. Pulmonary Failure H1. Specialty high-lipid low-carbohydrate formulations designed to manipulate the respiratory quotient and reduce CO 2 production are not recommended for routine use in ICU patients with acute respiratory failure. (This is not to be confused with guideline E2 for ARDS/ALI). H2. Fluid-restricted calorically dense formulations should be considered for patients with acute respiratory failure. H3. Serum phosphate levels should be monitored closely and replaced appropriately when needed. I. Renal Failure I1. ICU patients with acute renal failure (ARF) or acute kidney injury (AKI) should be placed on standard enteral formulations, and standard ICU recommendations for protein and calorie provision should be followed. If significant electrolyte abnormalities exist or develop, a specialty formulation designed for renal failure (with appropriate electrolyte profile) may be considered. I2. Patients receiving hemodialysis or continuous renal replacement therapy (CRRT) should receive increased protein, up to a maximum of 2.5 g/kg/d. Protein should not be restricted in patients with renal insufficiency as a means to avoid or delay initiation of dialysis therapy. J. Hepatic Failure J1. Traditional assessment tools should be used with caution in patients with cirrhosis and hepatic failure, as these tools are less accurate and less reliable due to complications of ascites, intravascular volume depletion, edema, portal hypertension, and hypoalbuminemia. J2. EN is the preferred route of nutrition therapy in ICU patients with acute and/or chronic liver disease. Nutrition regimens should avoid restricting protein in patients with liver failure. J3. Standard enteral formulations should be used in ICU patients with acute and chronic liver disease. Branched chain amino acid formulations (BCAA) should be reserved for the rare encephalopathic patient who is refractory to standard treatment with luminal acting antibiotics and lactulose. - 12 -
민명숙 : Recent Advances in ASPEN K. Acute Pancreatitis K1. On admission, patients with acute pancreatitis should be evaluated for disease severity. (Grade: E) Patients with severe acute pancreatitis should have a nasoenteric tube placed and EN initiated as soon as fluid volume resuscitation is complete. K2. Patients with mild to moderate acute pancreatitis do not require nutrition support therapy (unless an unexpected complication develops or there is failure to advance to oral diet within 7 days). K3. Patients with severe acute pancreatitis may be fed enterally by the gastric or jejunal route. K4. Tolerance to EN in patients with severe acute pancreatitis may be enhanced by the following measures: Minimizing the period of ileus after admission by early initiation of EN. (Grade: D) 맺음말 여러 연구들을 통해 정맥을 통한 영양공급보다 장 관을 통한 경장영양이 점막위축과 담관 및 췌장기능 부전을 예방하여 위장계의 기능을 유지하고, 감염 합 병증이나 수술적 중재를 감소시키고 비용효과측면에 서도 우수하다는 보고가 많아 경장영양의 조기 공급 을 강조하고 있으며, 2009년 발표된 Enteral Nutritin Practice Recommendations을 통해 안 전한 경장영양의 공급을 위한 처방, 라벨링과 formula의 안전성과 안정성, 약물투여 및 모니터링 등 의 권장사항을 상세하게 규정하고 추천하고 있다. 최 근에는 ASPEN에서 안전한 경장영양 공급을 위한 캠페인(BE A.L.E.R.T, BE A.W.A.R.E)을 활발히 벌이고 있으므로 우리도 임상 현장에서의 적극적인 활용을 고려해볼 수 있다. Displacing the level of infusion of EN more distally in the GI tract. Changing the content of the EN delivered from intact protein to small peptides, and long-chain fatty acids to medium-chain triglycerides or a nearly fat-free elemental formulation. Switching from bolus to continuous infusion. K5. For the patient with severe acute pancreatitis, when EN is not feasible, use of PN should be considered. PN should not be initiated until after the first 5 days of hospitalization. L. Nutrition Therapy in End-of-Life Situations L1. Specialized nutrition therapy is not obligatory in cases of futile care or end-of-life situations. The decision to provide nutrition therapy should be based on effective patient/family communication, realistic goals, and respect for patient autonomy. - 13 -